
Page 124 - Dementia-Care-Specialist-Toolkit
P. 124
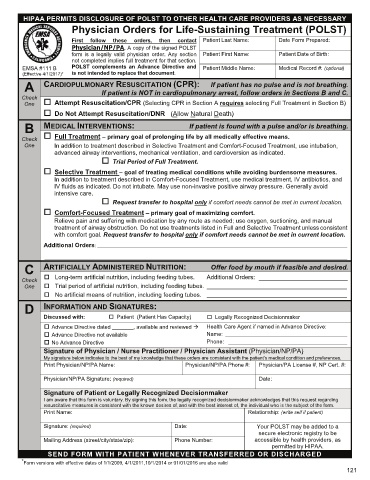
HIPAA PERMITS DISCLOSURE OF POLST TO OTHER HEALTH CARE PROVIDERS AS NECESSARY
Physician Orders for Life-Sustaining Treatment (POLST)
First follow these orders, then contact Patient Last Name: Date Form Prepared:
Physician/NP/PA. A copy of the signed POLST
form is a legally valid physician order. Any section Patient First Name: Patient Date of Birth:
not completed implies full treatment for that section.
EMSA #111 B POLST complements an Advance Directive and Patient Middle Name: Medical Record #: (optional)
e
4
t
i
v
1
/
17)
2
/
c
( (Effective 4/1/2017)** is not intended to replace that document.
Ef
0
e
f
A CARDIOPULMONARY RESUSCITATION (CPR): If patient has no pulse and is not breathing.
Check If patient is NOT in cardiopulmonary arrest, follow orders in Sections B and C.
One Attempt Resuscitation/CPR (Selecting CPR in Section A requires selecting Full Treatment in Section B)
Do Not Attempt Resuscitation/DNR (Allow Natural Death)
B MEDICAL INTERVENTIONS: If patient is found with a pulse and/or is breathing.
Check Full Treatment – primary goal of prolonging life by all medically effective means.
One In addition to treatment described in Selective Treatment and Comfort-Focused Treatment, use intubation,
advanced airway interventions, mechanical ventilation, and cardioversion as indicated.
Trial Period of Full Treatment.
Selective Treatment – goal of treating medical conditions while avoiding burdensome measures.
In addition to treatment described in Comfort-Focused Treatment, use medical treatment, IV antibiotics, and
IV fluids as indicated. Do not intubate. May use non-invasive positive airway pressure. Generally avoid
intensive care.
Request transfer to hospital only if comfort needs cannot be met in current location.
Comfort-Focused Treatment – primary goal of maximizing comfort.
Relieve pain and suffering with medication by any route as needed; use oxygen, suctioning, and manual
treatment of airway obstruction. Do not use treatments listed in Full and Selective Treatment unless consistent
with comfort goal. Request transfer to hospital only if comfort needs cannot be met in current location.
Additional Orders: ___________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
C ARTIFICIALLY ADMINISTERED NUTRITION: Offer food by mouth if feasible and desired.
Check Long-term artificial nutrition, including feeding tubes. Additional Orders: ________________________
One Trial period of artificial nutrition, including feeding tubes. __________________________________________
No artificial means of nutrition, including feeding tubes. __________________________________________
D INFORMATION AND SIGNATURES:
Discussed with: Patient (Patient Has Capacity) Legally Recognized Decisionmaker
Advance Directive dated _______, available and reviewed Æ Health Care Agent if named in Advance Directive:
Advance Directive not available Name: ________________________________________
No Advance Directive Phone: _______________________________________
Signature of Physician / Nurse Practitioner / Physician Assistant (Physician/NP/PA)
My signature below indicates to the best of my knowledge that these orders are consistent with the patient’s medical condition and preferences.
Print Physician/NP/PA Name: Physician/NP/PA Phone #: Physician/PA License #, NP Cert. #:
Physician/NP/PA Signature: (required) Date:
Signature of Patient or Legally Recognized Decisionmaker
I am aware that this form is voluntary. By signing this form, the legally recognized decisionmaker acknowledges that this request regarding
resuscitative measures is consistent with the known desires of, and with the best interest of, the individual who is the subject of the form.
Print Name: Relationship: (write self if patient)
Signature: (required) Date: Your POLST may be added to a
secure electronic registry to be
Mailing Address (street/city/state/zip): Phone Number: accessible by health providers, as
permitted by HIPAA.
SEND FORM WITH PATIENT WHENEVER TRANSFERRED OR DISCHARGED
* Form versions with effective dates of 1/1/2009, 4/1/2011,10/1/2014 or 01/01/2016 are also valid
121