
Page 20 - Dementia-Care-Specialist-Toolkit
P. 20
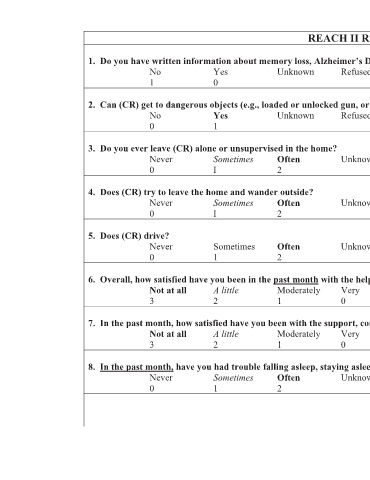
REACH II Risk Appraisal
1. Do you have written information about memory loss, Alzheimer’s Disease, or dementia?
No Yes Unknown Refused
1 0
2. Can (CR) get to dangerous objects (e.g., loaded or unlocked gun, or sharp objects that are used as weapons)?
No Yes Unknown Refused
0 1
3. Do you ever leave (CR) alone or unsupervised in the home?
Never Sometimes Often Unknown Refused
0 I 2
4. Does (CR) try to leave the home and wander outside?
Never Sometimes Often Unknown Refused
0 I 2
5. Does (CR) drive?
Never Sometimes Often Unknown Refused
0 1 2
6. Overall, how satisfied have you been in the past month with the help you have received from family members, friends, or neighbors?
Not at all A little Moderately Very Unknown Refused
3 2 1 0
7. In the past month, how satisfied have you been with the support, comfort, interest and concern you have received from others?
Not at all A little Moderately Very Unknown Refused
3 2 1 0
8. In the past month, have you had trouble falling asleep, staying asleep, or waking up too early in the morning?
Never Sometimes Often Unknown Refused
0 1 2
20